
![]()
Benjamin Alcock
Benjamin Alcock (1801 – ? ) was an Irish anatomist.
Alcock was the first Professor of Anatomy and Physiology at Queen’s College, Cork. However, he was forced to resign following a dispute over the 1832 Anatomy Act by conveying his disapproval regarding the procurement of corpses for the school.
Alcock coined the eponymous anatomical description of the pudendal canal; housing the internal pudendal artery, internal pudendal veins and the pudendal nerve. This has eponymously been named Alcock’s canal
Biography
- Born in May 1801 in the town of Kilkenny, Ireland
- 1819 – Scholarship to study anatomy under James Macartney (1770-1843) at Trinity College in Dublin. Unpaid apprenticeship under the skilled anatomist and surgeon, Abraham Colles (1773-1843)
- 1821 – BA, Trinity College in Dublin
- 1825 – Demonstrator of Anatomy at Park Street School in Dublin; Licentiate of the Royal College of Surgeons in Ireland.
- 1827 – M.B, University of Dublin; Member of the Royal College of Surgeons in Ireland
- 1836 – Lecturer in anatomy at the Peter Street School, Dublin
- 1837-1849 Professor of Anatomy, Physiology, and Pathology at the Apothecaries’ Hall on Cecilia Street, Dublin
- 1844 – M.D, and Fellow of the Royal College of Surgeons in Ireland.
- 1849-1854 First Professor of Anatomy and Physiology at Queen’s College, Cork
- 1854 – Forced to resign as Professor of Anatomy at Queen’s College following a dispute over the procurement of corpses for dissection.
The Murder Act of 1752 allowed only the corpses of executed murderers to be used for the medical schools’ dissections. However with the opening of more medical schools and the reduction in executions – there became a shortage of fresh cadavers.
This led to a lucrative trade in corpses as grave robbing became big business. But even this was not enough to serve the demand of the medical schools. A group of body snatchers (the London Burkers) came to prominence in 1831 following the murder of a 14 year old boy they were unable to sell to the medical schools.
The resurrection men, John Bishop (aged 33) and Thomas Williams (26) were convicted of murder with the intent to sell the corpses to London medical schools. In his confession, Bishop admitted to stealing (and selling) between 500-1,000 bodies over a period of twelve years
The Anatomy Act of 1832 established an Inspectorate to oversee the manner in which the schools procured corpses and to allow an authorized person to donate a corpse that they lawfully possessed. This further reduced the flow of corpses to medical schools, increasing the risk of illegal activities.
Alcock strongly disapproved of requests to participate in the illegal procurement of corpses. Professor O’Connor and Sir John Long, (who held the greatest authority under the Anatomy Act in Ireland) suggested to Alcock that he might “obtain subjects from the poorhouse by claiming bodies in the capacity of a friend of the deceased”.
When Alcock failed to agree to this suggestion he was forced to resign but petitioned to the Queen who passed the matter on to the Lord Lieutenant of Ireland who failed to pursue the matter further given the Earl of St German had already made a ruling on the matter.
- 1855 – Alcock formally dismissed
- 1859 – Departed for America, never to be heard of again…
Medical Eponyms
Alcock’s canal (1836)
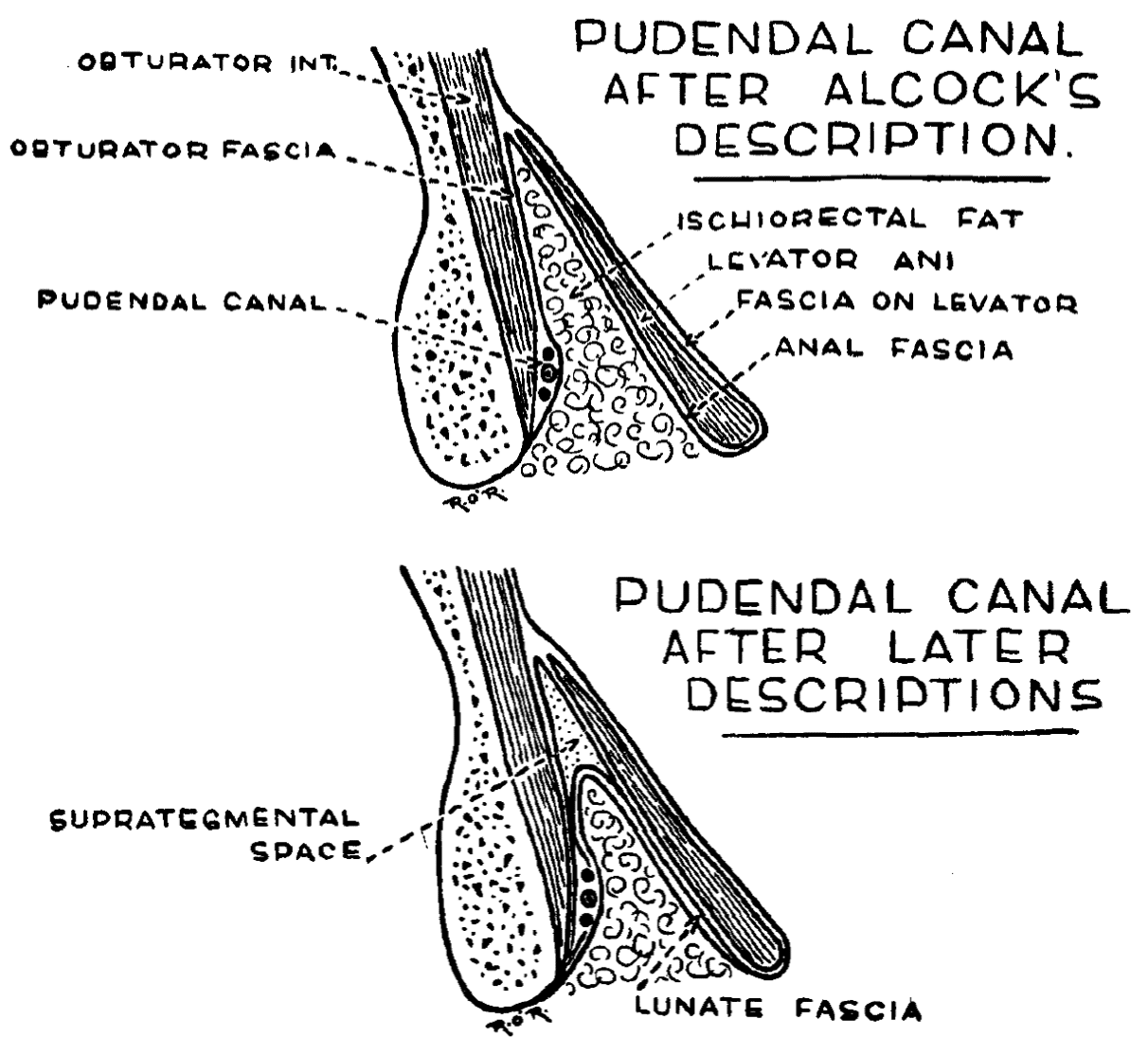
The description he gave of the sheath enclosing the pudendal nerve and internal pudendal vessels is his most famous contribution to the literature.
1836 – Alcock described the canal as being “in the obturator fascia”, and his original description was later modified.
In a canal in the obturator fascia the artery [internal pudendal] is contained through the posterior part of the third [perineal] stage ; by some it is maintained to be between the fascia and the muscle, in a sort of canal formed internally [medially] by the fascia, externally [laterally] by the muscle anti tuberosity, and inferiorly by the great sciatic [sacrotuborous] ligament ; but this is not correct ; the vessel being in the fascia, and not external [lateral] to it ; the line of its course is convex downward, about an inch and a half from the under surface of the tuberosity of the ischium at its most depending part, and from two to two and a half inches from the surface, this distance varying of course according to the condition of the subject ; the line approaches the margin of the ramus or the spinous process thence forward or backward.
Canalis pudendalis. In: Todd’s Cyclopaedia (1836-1839), Vol II: p835.
The canal was not referred to in the Nomina Anatomica, nor in the Jena nomina amatomiea of 1895. here it is termed Canalis pudendalis, after its contained vessels.
1907 – Douglas E. Derry, Assistant Professor of Anatomy of the Government School of Medicine in Cairo, found a further fascial layer which he named the “fascia lunata“. This he described as:
…a very dense crescentic mass of fibrous tissue which covers in the lowest, most ventral portion of the obturator internus muscle. This structure, which I have called the fascia lunata, is actually that part of the obturator fascia which forms the outer [lateral] wall of the ischio-rectal fossa, and encloses the pubic vessels and nerve [internal pudendal vessels and pudendal nerve] in a sheath usually known as Alcock’s canal
Derry 1907
Clinical Significance of Alcock’s canal
Pudendal neuralgia is a painful neuropathy that occurs when the pudendal nerve is injured, irritated or compressed. This can result from surgical procedures, pregnancy, childbirth, tumours, trauma, infections like herpes simplex and certain activities like cycling and squatting.
Pudendal neuralgia results in a burning or altered sensation (often unilateral) to the buttocks, genitals or perineum which is typically exacerbated by sitting and relieved on standing and lying flat. There is often associated dyspareunia, as well as, urgency and frequency to urinate and defecate.
This condition is also sometime referred to as Alcock’s syndrome or Pudendal nerve entrapment.
Treatment options include lifestyle modification, neuropathic analgesia, pudendal nerve block, and surgical decompression.
Major Publications
- Alcock B. Femoral artery. In: The Cyclopaedia of anatomy and physiology, Todd RB. (ed.) 1836–1839; Vol II: 235-257
- Alcock B. Fifth pair of nerves. In: The Cyclopaedia of anatomy and physiology, Todd RB. (ed.) 1836–1839; Vol II: 268-316
- Alcock B. Fourth pair of nerves. In: The Cyclopaedia of anatomy and physiology, Todd RB. (ed.) 1836–1839; Vol II: 370-371
- Alcock B. Iliac arteries. In: The Cyclopaedia of anatomy and physiology, Todd RB. (ed.) 1836–1839; Vol II: 827-850 [Alcock canal p835]
Controversies
The common ascription of the pudendal canal has been incorrectly to Thomas Alcock, M.D. (1784-1833)
References
Biography
- Medical News. The Lancet, 1848; 54(1362): 384
- O’Rahilly R. Benjamin Alcock, anatomist. Irish Journal of Medical Science, 1947; 22: 622–632
- O’Rahilly R. Benjamin Alcock : the first professor of anatomy and physiology in Queen’s College, Cork. 1948
- Oelhafen K, Shayota BJ, Muhleman M, Klaassen Z, Tubbs RS, Loukas M. Benjamin Alcock (1801-?) and his canal. Clin Anat. 2013; 26(6): 662-666.
- Baskett TF. Alcock, Benjamin. In: Eponyms and Names in Obstetrics and Gynaecology. 3e. 2019: 2
Eponymous terms
- His W, Sr. Die anatomische Nomenclatur. Nomina anatomica. 1895
- Derry DE. On the real nature of the so-called “pelvic fascia”. Journal of Anatomy and Physiology. 1907; 42: 97-106
- Derry DE. Pelvic muscles and fasciae. Journal of Anatomy and Physiology. 1907; 42: 107-111
- Buttner R. De-eponymising anatomical terminology. LITFL

Graduated from Leeds University in 2014 with MBChB and BSC in Primary Care. Qualified as a General Practitioner under RCGP in 2020. Currently working as an Emergency Department doctor in Sir Charles Gairdner Hospital in Perth, Australia.